

Laryngectomy: What it is and how it affects the quality of life.
May 07, 2026Laryngeal surgery represents a spectrum of interventions ranging from organ-preservation techniques to complete removal, depending on the extent of the disease. Whether partial or total, the primary goal is oncological safety removing the cancer while the secondary goal is the preservation or rehabilitation of vital functions: speech, respiration, and swallowing.
Types of laryngeal surgeries
Conservative laryngeal surgeries, also referred to as partial laryngectomies, allow for treatment of early glottic and supra-glottic cancers. This is heavily dependent upon the tumor location and involvement of surrounding structures. In the traditional setting, these conservative laryngeal surgeries are performed via an open approach involving trans-cervical exposure, resection, and reconstruction. With the advances in endoscopic and laser surgery, many early glottic and supraglottic tumors are now being treated with transoral laser microsurgery. Open partial laryngectomies, however, remain a critical surgical tool for patients that cannot be exposed endoscopically and for tumors that cannot be accessed with microsurgical techniques.
It includes two types; 1- Vertical partial laryngectomy (VPL) and horizontal partial laryngectomy (OPHL), they represent two distinct surgical approaches, each modifying the pharyngo-laryngeal anatomy in unique ways.
The vertical partial laryngectomy (VPL) is an approach focused on lesions originating at the glottic level and is defined by the removal of a portion or the entirety of a vocal fold along with the thyroid cartilage as the deep margin. A vertical transection through the thyroid cartilage is employed to allow for efficient access to the endolarynx. The extent of resection can vary from the simple excision of one vocal fold to as much as five-eighths of the larynx. In its simplest form, removal of one vocal fold can be performed via a midline thyrotomy incision.
An advantage of this approach is that a variety of reconstructive techniques are available. Postoperatively, patients should expect some degree of permanent hoarseness. However, this can vary depending on the reconstructive technique.
Another advantage of the VPL is the lack of postoperative chronic dysphagia.
92% of patients resumed a normal postoperative diet within 1 month of their surgery (Rademaker et al., 1993). Given the decrease in aspiration after VPL compared to other techniques, the tracheostomy tube can also often be deflated sooner than after supraglottic laryngectomy 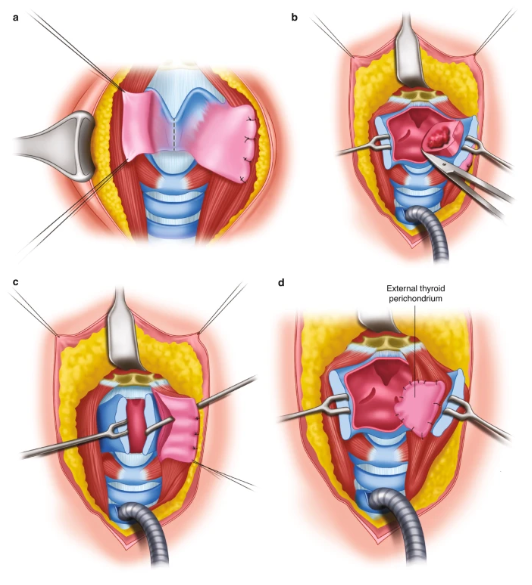
|
A horizontal partial laryngectomy, also commonly known as a supraglottic laryngectomy, involves the surgical resection of the structures above the true vocal folds, including the epiglottis, false vocal folds, and the superior portion of the thyroid cartilage. This procedure is primarily indicated for tumors localized in the supraglottic region, allowing the patient to retain their natural voice since the true vocal folds remain intact. However, because the "lid" of the larynx (the epiglottis) is removed, the primary clinical challenge is the significant risk of postoperative aspiration.
Horizontal Partial Laryngectomy (HPL), or Supraglottic Laryngectomy, offers specific advantages rooted in the fact that the "floor" of the larynx (the true vocal folds) is completely preserved. Unlike vertical partial laryngectomies or total laryngectomies, this procedure targets the structures above the vocal cords. Because the true vocal folds and the arytenoid cartilages are typically preserved, the patient’s natural phonation mechanism remains intact: The voice usually remains clear and strong, avoiding the permanent hoarseness associated with vertical partial laryngectomies
|
Although a temporary tracheostomy is almost always performed during surgery to manage postoperative swelling, the vast majority of HPL patients are successfully decannulated: Patients return to breathing entirely through their nose and mouth. This maintains the natural "nasal cycle," which filters and warms the air before it reaches the lungs, reducing the risk of crusting and chronic bronchitis seen in total laryngectomy patients.
Total laryngectomy is the surgical procedure in which the larynx is totally removed and the airway is interrupted, respiration being performed through a tracheal stoma resulting from bringing the trachea to the skin in the lower, anterior, cervical area. This provides a complete and permanent separation of the superior part of the airway from the inferior one, resulting in voice and smell loss. This surgery is addressed, mainly, to advanced laryngeal malignancy or malignancy of adjacent anatomical structures.
Total laryngectomy has dramatic consequences on the patient, mainly through the loss of speech, an essential social function, loss of smell and the possibility of heating, humidifying and filtering the inhaled air and finally through the impact the tracheal stoma has over the patient or society.
In addition, total laryngectomy fundamentally alters the anatomy of the neck, creating a complete physical separation between the digestive and respiratory tracts. Regarding respiration, the trachea is diverted to a permanent stoma in the neck, meaning the patient no longer breathes through the nose or mouth; this loss of nasal passage filtration necessitates artificial humidification to prevent pulmonary crusting. In terms of speech, the removal of the vocal folds results in a total loss of natural phonation, requiring the adoption of alaryngeal communication methods such as a tracheoesophageal prosthesis (TEP) or an electrolarynx. Swallowing is also impacted; while the risk of aspiration is eliminated because the airway is sealed off from the esophagus, many patients experience dysphagia due to reduced pharyngeal pressure, scar tissue strictures, or cricopharyngeal spasms.
Dissection and alteration of the cervical musculature:
The surgical management of laryngeal malignancy whether performed as a total or partial laryngectomy is never a localized procedure. It invariably necessitates a profound reconfiguration of the cervical musculoskeletal framework. To gain adequate visualization of the larynx and ensure oncological clearance, surgeons must navigate, dissect and retract multiple layers of the neck. This typically includes the mobilization or resection
- Platysma: This superficial muscle is typically incised as part of the initial skin flap (often using the Gluck-Sorenson U-shaped incision) to provide access to the deeper structures.
Injury to the platysma primarily affects:
Neck Mobility and Scarring: Damage can lead to skin contractures
and a decreased range of motion in the neck.
Lymphedema: Because the platysma is closely linked to the
superficial lymphatic drainage, its dissection often contributes to post-
operative swelling or "turkey wattle" edema under the chin.
- Infrahyoid Muscles (Sternohyoid and Sternothyroid): Often referred to as "strap muscles," these are generally divided or resected during the procedure. Since they lie directly over the larynx and are often involved in the surgical margins of the tumor, they are removed.
Since these "strap muscles" are typically resected, their loss results in:
Loss of Laryngeal Depression: These muscles normally pull the
larynx down. Without them, the remaining structures in the neck can
become stiff or develop fibrosis, leading to a "tight" sensation in the
throat.
Reduced Pharyngeal Clearance: They help stabilize the pharynx
during swallowing. Their absence contributes to pharyngeal residue,
where food remains in the throat after a swallow because the
"pumping" action is weakened.
- Suprahyoid Muscles: Muscles such as the mylohyoid and geniohyoid are often detached from the hyoid bone (which is typically removed in a total laryngectomy). This detachment weakens the structural support of the floor of the mouth, contributing to the "pumping" difficulty patients feel during the pharyngeal phase of swallowing.
The detachment or injury of these muscles significantly affects the "floor of the mouth":
Weakened Bolus Propulsion: These muscles are responsible for
pulling the tongue base and larynx upward and forward. Without this
support, patients often struggle to "push" the food back into the
esophagus, leading to multiple swallows being needed for a single
bite.
Reduced UES Opening: The upward pull of the suprahyoids is what
physically pulls the Upper Esophageal Sphincter (UES) open. Injury
here often leads to cricopharyngeal dysfunction, where the "door"
to the esophagus doesn't open wide enough.
- Sternocleidomastoid (SCM): While the main belly of the SCM is usually retracted laterally and preserved, its sternal heads may be released to flatten the neck for better
Even if the muscle is only retracted or the sternal heads are released, the impact is noticeable:
Postural Imbalance: Injury can lead to "Dropped Head Syndrome" or
a tilted posture, as the SCM is a primary stabilizer for head rotation
and flexion.
Laryngectomy and quality of life :
Individuals who have had a TL have reduced QoL compared with published norms, They had significantly reduced physical health QoL and social relationships QoL when compared with age and gender matched normative data from the WHOQoL-Bref.
After experiencing a diagnosis of laryngeal cancer and then undergoing TL surgery with its associated impairment, a person's perceptions of their physical health is (unsurprisingly) reduced . Their burden of disease includes having ongoing dependence on treatments, experiencing increased pain, discomfort and fatigue, and participation at work and in activities of daily living may be significantly reduced from their pre-morbid status
Lowered social relationship QoL is not unexpected in individuals who have had a TL. People after TL often experience barriers to fulfilling relationships with others, especially where there are limitations to their speech and swallowing, In one published study, 40% of 218 patients who had a TL reportedly withdrew from social conversations and 70% did not partake in regular social activities . Perceived stigmatization related to changed voice and use of a tracheostoma was also common

|
The “pulmonary issues” seem to have a strong correlation to most other themes. Therefore these pulmonary issues might be partially responsible for other reported issues. Although reported less frequently, the issues from the two themes “avoiding social activities” and “experienced limitations in daily activities” are the main influencers of the variance in r-QoL. Thus, the ability to fulfill meaningful activities seems to have a greater impact on r-QoL than the purely physical consequences of TL in general.
A laryngectomy whether partial or total is a life-altering intervention that extends far beyond the removal of a tumor. While surgical advancements in vertical and horizontal partial laryngectomies have paved the way for organ preservation and functional maintenance, the "reconstructed neck" remains an anatomical challenge. The inevitable dissection of the cervical musculature and the redistribution of lymphatic pathways create a complex landscape for recovery.
As we have explored, the impact on a patient’s quality of life is profound, touching upon the most fundamental human functions: breathing, speaking, and swallowing. The transition from natural phonation to alaryngeal communication, the management of a permanent stoma, and the struggle with postoperative dysphagia and lymphedema represent a significant physical and psychosocial burden. However, understanding the intricate relationship between surgical techniques and muscular alterations is the first step toward effective rehabilitation. For the clinician and the patient alike, the ultimate goal remains clear: to move beyond oncological survival toward a meaningful restoration of function and social reintegration.
References:
1- Ceachir O, Hainarosie R, Zainea V. Total laryngectomy - past, present, future. Maedica (Bucur). 2014 Jun;9(2):210-6. PMID: 25705281; PMCID: PMC4296768.
2- Chotipanich A. Total Laryngectomy: A Review of Surgical Techniques. Cureus. 2021 Sep 22;13(9):e18181. doi: 10.7759/cureus.18181. PMID: 34707956; PMCID: PMC8531883.
3- Thurnher D, Simo R, Succo G, Vilaseca I and Simon C (2025) Open partial or transoral laryngectomy – total laryngectomy today. Front. Oncol. 15:1520524. doi: 10.3389/fonc.2025.1520524
4- Evangelista, L. M. (Ed.). (2023). Total Laryngectomy: Assessment and Management of Respiration, Swallowing, and Alaryngeal Voice. Plural Publishing.
5- Zenga, J., T. Goldsmith, G. Bunting, and D.G. Deschler, “State of the art: Rehabilitation of speech and swallowing after total laryngectomy,” Oral Oncology, 86, pp. 38–47 (2018).
6- eleyiannis, F.W.-.-B., Weymuller, E.A., Jr., Coltrera, M.D. and Futran, N. (1999), Quality of life after laryngectomy: Are functional disabilities important?. Head Neck, 21: 319-324.
7- Perry, A., Casey, E. and Cotton, S. (2015), Quality of life after total laryngectomy: functioning, psychological well-being and self-efficacy. INT J LANG COMMUN DISORD, 50: 467-475.
8- Leemans M, vanSluis KE, vanSon RJJH, van denBrekel MWM. Interaction of functional and participation issues on quality of life after total laryngectomy. Laryngoscope Investigative Otolaryngology. 2020;5:453–460.
Stay connected with news and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
We hate SPAM. We will never sell your information, for any reason.
