

The Functional Triad: Dysphagia, Pulmonary Health, and Communication Post-Laryngectomy
May 08, 2026Dysphagia after laryngectomy
Following a laryngectomy, dysphagia remains one of the most prevalent and complex challenges, significantly impacting a patient's nutritional status and overall quality of life. Postoperative swallowing difficulties are multifactorial in nature, arising from a combination of structural alterations, functional deficits.
After removal of the larynx, the resulting defect of the pharynx is repaired, creating the so-called neopharynx. The ideal neopharynx must be watertight to avoid leakage, sufficiently large to allow food passage, and capable of accommodating voice rehabilitation
Patients requiring circumferential pharyngeal resection have an increased incidence of neopharyngeal stenosis and slow pharyngeal bolus transit, particularly in the distal anastomotic region, and resulting dysphagia as compared with those undergoing only partial pharyngectomy . These patients often complain of obstruction of solid foods and medications and slow transit of liquids causing reduced oral intake and increased duration of mealtimes
Early VFS picture showing aspiration for patient underwent supracricoid laryngectomy with cricohyoidoepiglottopexy. ( Subramaniam et al. 2018 )

Various neopharyngeal findings after primary pharynx closure were reported as contributing to dysphagia . Among these, the main ones were impaired pharyngeal propulsion,i ncreased pharyngeal outflow resistance, pharyngeal weakness, pharyngoesophageal dysfunction, pharyngoe-sophageal spasm, and nasopharyngeal reflux.
There are Specific anatomic deficits that occur after removal of the larynx. Along with the cartilages of the larynx, the hyoid bone is removed, which formerly contributed to hyolaryngeal elevation just prior to and during the swallow. The base of the tongue forms the upper anastomosis with the neopharynx for reconstruction leading to the pharyngoesophageal sphincter and joined by the closure of the layers of the cricopharyngeus muscles over the sphincter. As such, there may be limits in tongue base retraction either from weakness or decreased range of motion. McConnel (1988) found that higher tongue base to posterior pharyngeal wall pressures are required after laryngectomy to propel a bolus through the pharynx. In addition, the tonicity of the pharyngoesophageal segment, which acts as the upper esophageal sphincter (UES), is affected by the potential driving forces of the tongue base and hyolaryngeal elevation along with the basic tonus of the sphincter itself. As many of these structures have been altered and/or rearranged, relaxation of the sphincter is not as readily accomplished.
Fistulae may develop at any point after surgical excision, but most frequently occur in the first few weeks. Depending on the location, pharyngo-cutaneous, oro-cutaneous fistulae are more common in patients requiring more extensive resections. Patients are typically NPO while fistulae are present to reduce any flow through the fistula tract and to promote healing. Once the fistula is closed, diet progresses from liquids to denser consistencies as tolerated.
Pharyngeal clearance problems may exist after laryngectomy and adversely affect swallowing. This can then result in backflow of material into the pharynx during the swallow. Reduced pharyngeal clearance may be due to the loss of both superior and anterior motion previously accomplished by hyolaryngeal elevation and tongue base retraction that are required to assist opening of the UES. Potential causes for pharyngeal stasis include anything that might impair neuromuscular control of the pharyngeal wall or base of tongue musculature, including posttreatment edema and surgical resection impairing range and strength of palatal motion. Problems with pharyngeal clearance are evident when patients complain of feeling persistent material in their throats, regurgitate material they were attempting to swallow, and exhibit a wet, gurgly vocal quality.
Stricture (narrowing) may develop in the pharynx or esophagus and impede bolus passage. This is more commonly seen in the hypopharynx related to tight surgical closures. Prior radiation therapy and post-operative infections also may increase the likelihood of scarring and stricture formation. A stricture is suspected when patients evidence difficulties with denser consistencies of food along with a globus sensation and pooled materials in the pharynx. Another symptom of esophageal stricture is nasal regurgitation that occurs after the swallow. This is related to ineffective bolus passage through a narrowed area, with pooling or backflow of material in a retrograde manner through the nasopharynx after the swallow is complete and velopharyngeal closure has relaxed.
Pseudoepiglottis or a pseudodiverticulum may form and be additional complications to efficient swallowing. These abnormal pseudo-structures develop as a result of surgical healing along with scar development. pseudoepiglottis develops at the base of the tongue area. mimicking the appearance of an epiglottis. Due to lack of muscular presence, a pseudoepiglottis serves as an impediment to bolus passage. These may collect significant amounts of food while the patient is eating,
Patients will frequently complain of regurgitating undigested food or sensing the material for prolonged periods of time after eating and halitosis .
It remains unclear which surgical closure technique is the best for efficient swallowing, and that question needs further investigation. It was not possible to stratify swallowing outcomes per surgical technique due to a great variation in the methods used.
Communication after laryngectomy
Lowered social relationship QoL is not unexpected in individuals who have had a TL. People after TL often experience barriers to fulfilling relationships with others, especially where there are limitations to their speech and swallowing, The authors noted that contributing factors to the negative impact were the perceived difficulties and frustrations of participants with not being understood by familiar and unfamiliar listeners, the difficulties faced when talking on the telephone, as well as the physical difficulties of talking.
General changes to communication that were reported included being less able to:
(a) express aspects of their character and personality (e.g. communicating with greater effort and being less spontaneous)
(b) use humour in a timely way during conversation (e.g. engaging with humour before the conversational topic changed);
(c) be understood by unfamiliar listeners and perceived negatively by them (e.g. the reaction of others to the artificial sounding voice and participants being viewed as having reduced cognitive ability)
(d) be understood in noisy environments.
Due to these negative changes, the participants experienced avoidant behaviours during social interactions where communication was difficult for them (e.g. nodding to avoid small talk initiated by others or limiting their conversation), and feelings of loss of social status and avoiding social situations (e.g. preferring to help with the food preparation rather than mingling at a social event). Additionally, the participants reported going through a process of managing expectations of their communication ability (e.g. not expecting that communication interactions would improve with time); and having to cope and adapt to change. The changes were noted when socialising (e.g. mentally preparing prior and during the interaction, and having to let others know how they could better support the communication interaction), and to reactions of others (e.g. to the quality of the artificial voice or as participants blocked the stoma with the thumbs to communicate).
Pulmonary health after laryngectomy
Changes in the upper airway in patients following a total laryngectomy subsequently alter respiration balance result in compensatory alterations to breathing. The removal of laryngeal afferent input, greater upper airway resistance, and possible respiratory compromise may affect the flexibility necessary for maintaining homeostasis and for achieving proficient alaryngeal speech
Altered anatomy after laryngectomy Greatbatch, J. (2016).
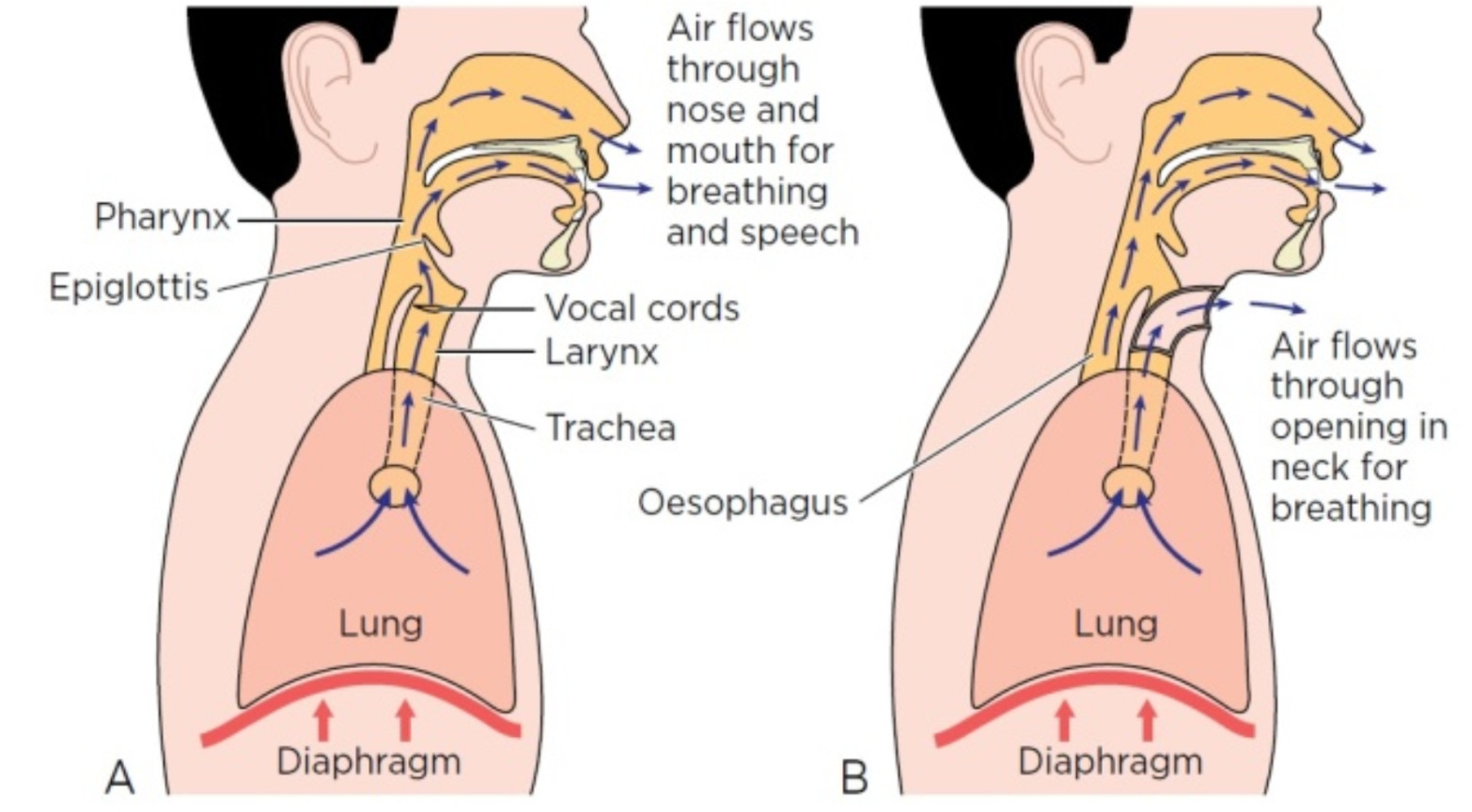
Total laryngectomy results in the removal of the larynx and superior laryngeal nerve (SLN) of cranial nerve (CN) X (vagus). The SLN may influence the timing and firing rate of the respiratory muscles, a process which aids in maintaining airway integrity. Airflow, pressure, mucosal temperature, and stretch receptor sensation are altered due to the loss of laryngeal afferent input,
These changes affect the gas exchange process at the alveoli level, and the heating, moisturizing and filtering of inhaled air , For the patient, these changes manifest as a persistent "laryngectomy bronchitis," increased coughing, and a heightened risk of mucous plugging (crusting), necessitating the lifelong use of Heat and Moisture Exchangers (HMEs) to simulate the lost functions of the upper airway.
Heat and moisture exchangers (HMEs) have been introduced to partly compensate for the deficits . They condition the inhaled air, thereby improving the tracheal climate and reducing the loss of water, they filter out larger particles, and increase both inhalatory and exhalatory breathing resistance , Several studies have demonstrated the positive pulmonary, psychosocial and voice and speech benefits of HME use experienced by laryngectomized patients The clinical effects of post-laryngectomy HME use can be divided into effects achieved by continuous, compliant use (improved pulmonary symptoms, such as coughing and forced expectoration, sleeping, psychosocial aspects), and more immediate effects that are noticeable directly after putting on the HME (airway effects, device related aspects such as hygienic stoma occlusion, ease of stoma occlusion, voice and speech). It is known that patients only experience the full benefits of an HME when it is used compliantly for a longer period of time
Vital capacities following a total laryngectomy are often less than 100% of their predicted value . Reports of VC as low as 2.5 L are common in laryngectomized patients, a volume that is approximately 50% of that expected for adult males . Reduced functional expiratory volume, reduced maximum expiratory flow, peak and mean expiratory flows, and reduced residual volume are all expected in the first year following the total laryngectomy
It is also evident that pulmonary issues have a great effect on quality of life of laryngectomy patients , it seems to have a strong correlation to most other themes. Therefore these pulmonary issues might be partially responsible for other reported issues; avoiding social activities, communication, sleep and limitation and daily activity
"Functional Triad" of dysphagia, pulmonary health, and communication represents the core challenges faced by patients following a laryngectomy. As we have examined, the transition to a life without a larynx is not merely a surgical outcome but a profound physiological and psychosocial shift. The development of a neopharynx, while necessary for survival, introduces complex swallowing mechanics where structural issues like strictures or pseudoepiglottis can significantly impede nutritional intake. Simultaneously, the loss of the upper airway’s natural conditioning functions necessitates lifelong pulmonary vigilance and the consistent use of Heat and Moisture Exchangers (HMEs) to preserve lung health and maintain vital capacity.
Ultimately, these physical alterations converge to impact the most human aspect of recovery: communication. The struggle to be understood in social settings, the loss of spontaneous humor, and the frustration of alaryngeal speech contribute to a reduced quality of life that often leads to social withdrawal. Therefore, the successful rehabilitation of a laryngectomy patient must be multidisciplinary. It requires not only surgical precision but also a dedicated focus on restoring functional integrity through targeted therapy. By addressing the pulmonary, digestive, and communicative needs as an interconnected system, we can empower patients to move beyond the limitations of their surgery and re-engage with the world around them.
References:
1- Landera, M.A., D.S. Lundy, and P.A. Sullivan, “Dysphagia After Total Laryngectomy,” Perspectives on Swallowing and Swallowing Disorders (Dysphagia), 19 (2), pp. 39–44 (2010).
2- Ceachir O, Hainarosie R, Zainea V. Total laryngectomy - past, present, future. Maedica (Bucur). 2014 Jun;9(2):210-6. PMID: 25705281; PMCID: PMC4296768.
3- Bohnenkamp, T.A. (2019). Postlaryngectomy Respiratory System and Speech Breathing. In: Doyle, P. (eds) Clinical Care and Rehabilitation in Head and Neck Cancer. Springer, Cham. https://doi.org/10.1007/978-3-030-04702-3_7
4- Herranz, J., Espiño, M.A. & Morado, C.O. Pulmonary rehabilitation after total laryngectomy: a randomized cross-over clinical trial comparing two different heat and moisture exchangers (HMEs). Eur Arch Otorhinolaryngol270, 2479–2484 (2013).
5- Sharpe, G., V. Camoes Costa, W. Doubé, J. Sita, C. McCarthy, and P. Carding, “Communication changes with laryngectomy and impact on quality of life: a review,” Quality of Life Research, 28 (4), pp. 863–877 (2018).
6- Chotipanich A. Total Laryngectomy: A Review of Surgical Techniques. Cureus. 2021 Sep 22;13(9):e18181. doi: 10.7759/cureus.18181. PMID: 34707956; PMCID: PMC8531883.
7- Terlingen, L.T., W. Pilz, M. Kuijer, B. Kremer, and L.W. Baijens, “Diagnosis and treatment of oropharyngeal dysphagia after total laryngectomy with or without pharyngoesophageal reconstruction: Systematic review,” Head & Neck, 40 (12), pp. 2733–2748 (2018).
8- Leemans M, vanSluis KE, vanSon RJJH, van denBrekel MWM. Interaction of functional and participation issues on quality of life after total laryngectomy. Laryngoscope Investigative Otolaryngology. 2020;5:453–460.
Stay connected with news and updates!
Join our mailing list to receive the latest news and updates from our team.
Don't worry, your information will not be shared.
We hate SPAM. We will never sell your information, for any reason.
